Mood Stabilizer Interaction Checker
Check Drug Interactions
Select a mood stabilizer and a common medication to see potential interactions and safety information.
When you're managing bipolar disorder, finding the right mood stabilizer isn't just about controlling highs and lows-it's about avoiding dangerous drug clashes that can land you in the hospital. Three older but still widely used medications-lithium, valproate, and carbamazepine-are powerful, but they don't play well with everything. Even common over-the-counter painkillers or blood pressure meds can turn safe doses into toxic ones. This isn't theoretical. Real people have ended up in emergency rooms because of these interactions, and many clinicians still miss the warning signs.
Why Lithium Is the Most Fragile
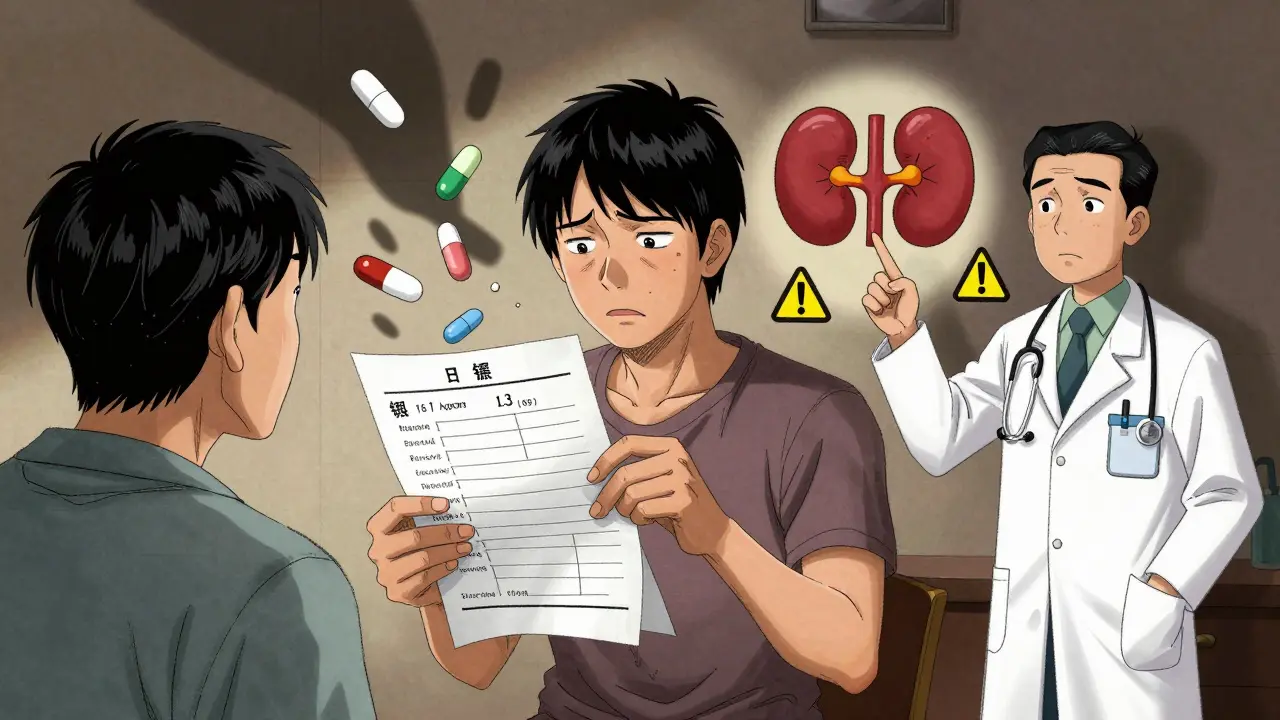
Lithium is simple in how it works, but that simplicity makes it dangerously easy to mess up. It leaves your body through your kidneys, and nothing else. That means anything that affects kidney function or sodium levels can cause lithium to build up to toxic levels. A 25% increase in lithium concentration might sound small, but in practice, it's enough to trigger tremors, confusion, or even seizures.NSAIDs like ibuprofen or naproxen are the most common culprits. A 1989 study showed these painkillers reduce lithium clearance by 25-30%. One patient on NAMI’s forum described going from a stable lithium level of 0.8 to 1.3 mmol/L after starting ibuprofen for a headache-symptoms kicked in within days. Thiazide diuretics, often prescribed for high blood pressure, can push lithium levels up by 25-40%. Even ACE inhibitors, which seem harmless, can raise lithium by about 25%.
There’s no workaround here. If you’re on lithium and your doctor prescribes any new medication, you need a blood test within 5-7 days. The goal isn’t just to avoid toxicity-it’s to keep levels low. Current guidelines recommend staying at the bottom of the therapeutic range (0.6-0.8 mmol/L) when taking interacting drugs. Hydration matters too. Dehydration, even mild, can spike lithium levels. That’s why doctors tell patients to drink water, avoid excessive caffeine, and skip saunas or intense workouts during hot weather.
Valproate: The Hidden Bidirectional Threat
Valproate doesn’t just affect your mood-it changes how your body handles other drugs. Unlike lithium, it’s metabolized in the liver through three different pathways, which makes it more stable, but also more unpredictable. It can both increase and decrease the levels of other medications, depending on what you’re taking.One of the most dangerous combos is valproate with lamotrigine. Valproate blocks the enzyme that breaks down lamotrigine, causing its levels to double or even triple. A Reddit user shared that when switching from carbamazepine to valproate, their lamotrigine dose had to be cut in half-from 400 mg to 200 mg-to avoid skin rashes and dizziness. That’s not a guess; it’s standard clinical practice backed by studies from 1994.
But valproate doesn’t just boost other drugs-it gets weakened too. Carbamazepine speeds up how fast your body clears valproate, cutting its levels by 30-50%. That means someone on both drugs might feel like their mood stabilizer stopped working, when in reality, their body is burning it off too fast. That’s why doctors check valproate levels when starting or stopping carbamazepine. It’s not enough to assume the dose is still right.
There’s another layer: valproate binds tightly to proteins in your blood. When levels go above 100 mcg/mL, that binding gets saturated, and free (active) drug levels can spike suddenly. This is why monitoring isn’t optional-it’s lifesaving. And while valproate is less likely to cause liver enzyme issues than carbamazepine, its biggest risk isn’t interaction-it’s pregnancy. A 2019 JAMA study found that 10.7% of babies born to mothers on valproate had major birth defects, compared to 2.6% in the general population. That’s why it’s avoided in women of childbearing age unless absolutely necessary.
Carbamazepine: The Metabolism Machine
Carbamazepine doesn’t just interact-it rewires your body’s drug-processing system. It’s an enzyme inducer, meaning it tells your liver to produce more of the enzymes that break down medications. After 3-5 weeks of use, your body starts clearing carbamazepine faster, which is why dose adjustments are often needed early on. But the real problem is what it does to other drugs.Carbamazepine slashes the effectiveness of oral contraceptives by 50-70%. Women on this drug who rely on birth control pills for contraception are at high risk of unintended pregnancy. It also reduces levels of antipsychotics like risperidone and haloperidol, which can cause psychosis to return. Even common antidepressants like sertraline can become less effective.
But the most complex interaction is with valproate. For years, doctors thought valproate increased carbamazepine toxicity by blocking one enzyme (epoxide hydrolase). New research from 1997 showed it’s more complicated: valproate also blocks the next step in the process, trapping the toxic metabolite (carbamazepine-epoxide) in your system. This metabolite causes dizziness, nausea, and loss of coordination. In fact, when both drugs are used together, epoxide levels can rise by 40-60%, even if carbamazepine levels look normal.
That’s why guidelines now recommend checking both carbamazepine and its epoxide metabolite levels when combining the two. A 25% reduction in carbamazepine dose is often needed at the start of valproate therapy. Without this, patients report feeling “drunk” or unsteady within days. A 2019 survey of 853 clinicians found 74% considered this interaction “moderately to severely problematic.”
What Happens When You Mix All Three?
Using lithium, valproate, and carbamazepine together is rare-but it happens. Usually, it’s after multiple medication failures. One 2022 case study followed a patient with rapid-cycling bipolar disorder who’d tried 12 other drugs without success. The team combined lithium and valproate, carefully monitoring both levels. Lithium stayed at 0.8 mmol/L, valproate at 95 mcg/mL. No toxicity. No hospitalizations. Eighteen months later, they were stable.But this isn’t a recipe for everyone. The risk is layered. Lithium is vulnerable to kidney stress. Valproate can interfere with lamotrigine or get cleared too fast. Carbamazepine can suppress other meds and build up toxic metabolites. The more drugs you stack, the harder it is to track what’s causing what.
That’s why most psychiatrists avoid triple combinations unless there’s no alternative. Even then, they use it as a last resort, with weekly blood tests at first, then monthly. It’s not about being aggressive-it’s about being precise.
Why These Drugs Are Losing Ground
You might wonder why these three are still around if they’re so tricky. The answer is cost and history. Lithium costs $30 a month. Valproate generics run about $50. Carbamazepine is similar. Newer drugs like lamotrigine or lurasidone cost $300-$500 a month. Insurance often pushes the older, cheaper options first.But usage is shifting. In 2012, lithium was prescribed in 35% of new mood stabilizer starts. By 2022, that dropped to 15%. Valproate fell from 55% to 40%, mostly because of pregnancy risks. Carbamazepine stayed steady at 10%. Lamotrigine, with fewer interactions and a better safety profile, now leads at 35%.
Even so, these three still have a place. Lithium is the only mood stabilizer proven to reduce suicide risk by nearly half. Valproate works fast in acute mania. Carbamazepine helps when other drugs fail. But their use demands vigilance.
What You Need to Do Right Now
If you’re on one of these drugs, here’s what matters:- Know your levels. Lithium, valproate, and carbamazepine all need regular blood tests. Don’t skip them, even if you feel fine.
- Tell every doctor you’re on a mood stabilizer. Even your dentist or primary care provider needs to know. A simple ibuprofen prescription can be dangerous.
- Watch for symptoms. For lithium: tremors, confusion, nausea, frequent urination. For valproate: drowsiness, swelling, unusual bleeding. For carbamazepine: dizziness, double vision, rash. Don’t wait for a blood test if you feel off.
- Don’t stop or change doses on your own. Abruptly stopping carbamazepine can trigger seizures. Suddenly stopping lithium can cause rebound mania.
- Ask about alternatives. If you’re on multiple interacting drugs, ask if a newer agent like lamotrigine or lurasidone might be safer for you.
These drugs aren’t obsolete. But they’re not simple. They require active partnership between you and your care team. The goal isn’t just to stabilize your mood-it’s to do it without risking your life in the process.
Priscilla Kraft
January 12, 2026 AT 04:12Just had my lithium level checked after my doc slipped me some ibuprofen for a migraine 🤦♀️ Turned out it spiked from 0.7 to 1.1 in 5 days. Learned the hard way - now I keep a list of safe OTC meds taped to my fridge. Seriously, if you're on lithium, treat every new pill like a landmine. Water. Water. Water. And maybe a little emoji for self-care: 💧🧠
Jennifer Littler
January 13, 2026 AT 05:32Valproate’s bidirectional pharmacokinetics are a nightmare in clinical practice. The CYP450 inhibition profile, particularly UGT1A6 and CYP2C9 suppression, coupled with protein binding saturation kinetics above 100 mcg/mL, creates nonlinear concentration-response curves that are virtually impossible to predict without TDM. The lamotrigine interaction is especially insidious - the 50% reduction in clearance isn’t linear, it’s exponential. Always validate with serum levels, never assume dose equivalence post-switch.
Sean Feng
January 15, 2026 AT 05:30Alex Smith
January 16, 2026 AT 05:56So let me get this straight - you’re telling me a guy on carbamazepine can get pregnant while on birth control, and his psychiatrist doesn’t notice? And we’re surprised people end up in the ER? I mean, this isn’t rocket science. It’s basic pharmacology. But hey, if you think your GP knows more than your psych med list, go ahead and trust them with your life. I’ll be over here, reading the FDA label. 🤷♂️
Adewumi Gbotemi
January 16, 2026 AT 09:48Roshan Joy
January 17, 2026 AT 03:47As someone who’s been on lithium for 8 years, I can say hydration is everything. I drink 3L of water daily, avoid coffee after noon, and skip gym on hot days. My doc says I’m lucky - my levels stay steady. But I know people who didn’t listen and ended up in ICU. Don’t be that person. Your stability is worth the effort. And yes, I still use ibuprofen - but only after checking with my psych team. Small steps save lives.
Michael Patterson
January 18, 2026 AT 14:46Matthew Miller
January 19, 2026 AT 14:52Oh great. Another ‘educational’ post from someone who clearly never had to manage their own meds. You think people don’t know this? We’ve been screaming about these interactions for years. The real problem? Doctors who don’t listen. Pharmacies that don’t flag. Insurance that pushes the cheapest crap. This isn’t about information - it’s about systemic neglect. And now you want a pat on the back for stating the obvious? Go write a textbook. We need action, not another lecture.
Madhav Malhotra
January 20, 2026 AT 17:03Coming from India - we have a lot of people on these meds because they’re cheap. But we also have zero access to regular blood tests. My cousin was on valproate and carbamazepine together for 2 years without any monitoring. He got dizzy, stopped driving, and thought it was ‘just stress’. No one told him it could be the drugs. This post should be translated and shared in every village clinic. Knowledge is power, but access is justice.
Priya Patel
January 22, 2026 AT 08:02I’m on lamotrigine now and honestly? I feel like a new person. No more scary blood tests, no more ‘oh btw your lithium just spiked’ panic. But I still keep this post saved because my mom is on lithium and I don’t want her to end up in the ER. Seriously, if you’re on one of these old-school meds, tell EVERYONE. Your dentist, your yoga instructor, your Uber driver (jk… maybe not them). But your doctor? Yeah. Tell them. And if they look confused? Print this out. 💖